
Coach Kolton built a following, at least in part, on being the guy who stepped back. After years of heavy roid use, he publicly committed to reversing course and cleaning up his act. So when his current cycle leaked online, it caught more than a few people off guard.
Greg Doucette broke down the leaked protocol in detail, and his verdict was blunt: “I think it’s st*pid. I think it’s going to be a net negative.”
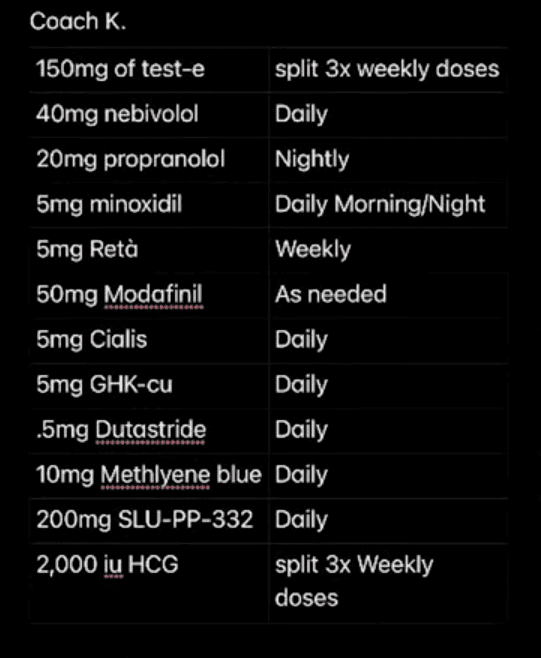
The cycle centers on 150mg of testosterone per week, split into three doses for more stable blood levels. Doucette said that part was reasonable, noting he himself runs 140mg weekly. The problems, in his view, start with everything layered on top.

Colton is also taking Retatrutide, a GLP/GIP agonist similar to Ozempic or Tirzepatide but not yet FDA approved, at 5mg. Doucette argued it makes no sense for someone already at single-digit body fat, saying it creates a situation where the body is constantly starved for energy.
He stated, “He has the testosterone. This is essentially like the workers building on your house. It’s a construction crew. Now, the nutrition, the protein, the calories, that is the boards and the nails. With more testosterone, you have more workers, but you got no boards and nails.”
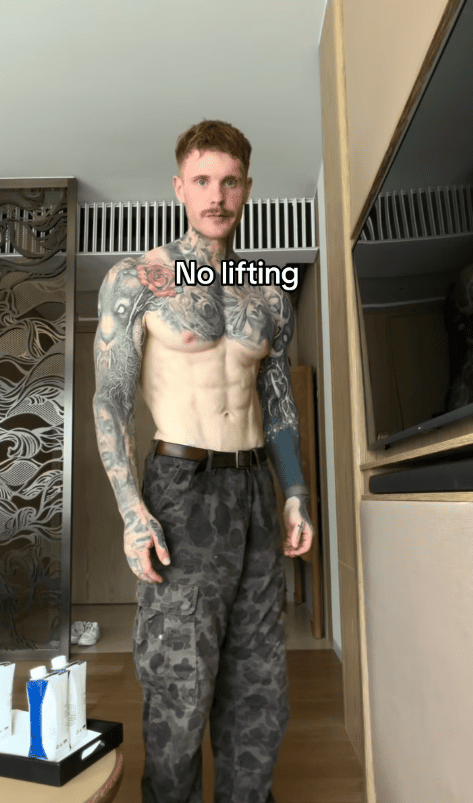
The result, Doucette argued, is that Kolton is now visibly smaller than when he was training without any enhancement. He described it as “looks minimizing.”

The blood pressure portion of the protocol drew the sharpest criticism. Colton is reportedly taking 40mg of nebivolol, 20mg of propranolol nightly, and 5mg of oral minoxidil. Doucette pointed out that studies on nebivolol show no benefit beyond 5mg, and that layering three blood pressure treatments simultaneously is outright dangerous.
“When you combine propranolol, nebivolol, and minoxidil in that combination, it’s too much. It’s dangerous. His previous doses of roids was probably safer than this,” he stated.
The propranolol at night, Doucette noted, is a dose typically used for akathisia, a condition marked by restlessness that can be triggered by antipsychotic treatments, raising questions about what else Colton may be managing.
Rounding out the stack: 50mg of modafinil for energy, 5mg GHK-CU, 5mg dutasteride daily, 10mg methylene blue, 200mg of SLU-PP-332, and 2,000 IUs of HCG three times per week.
Doucette flagged methylene blue as carrying a real risk of serotonin syndrome and questioned why HCG would be included at a stage where the body is already under significant caloric stress.
His overall read was that the cycle looks self-prescribed, calling it a “polypharmacy” stack that no responsible physician would put together without ongoing monitoring. “I don’t believe that any doctor would prescribe this.”
For someone who positioned himself as a cautionary voice on PED protocols, the leaked cycle suggests Colton’s approach has become considerably more complex than the simplified TRT story he had been telling publicly.